
Tubular Breast Correction in San Francisco: What to Know Before Surgery
Overview
Tubular breasts (also called tuberous breasts) are a congenital condition where breast tissue doesn't develop normally during puberty, leaving a narrow base, enlarged areolas, and a tube-like shape.
Most patients describe breasts that look small and saggy despite no weight changes and no childbirth
A standard augmentation won't fix this. The internal tissue needs to be released first through a technique I call "pie cuts"
Correction involves tissue release, silicone gel implants, areolar reduction, and sometimes fat grafting, all through an areolar incision
Final results take 6 to 12 months. Some patients need a smaller secondary procedure for fine-tuning
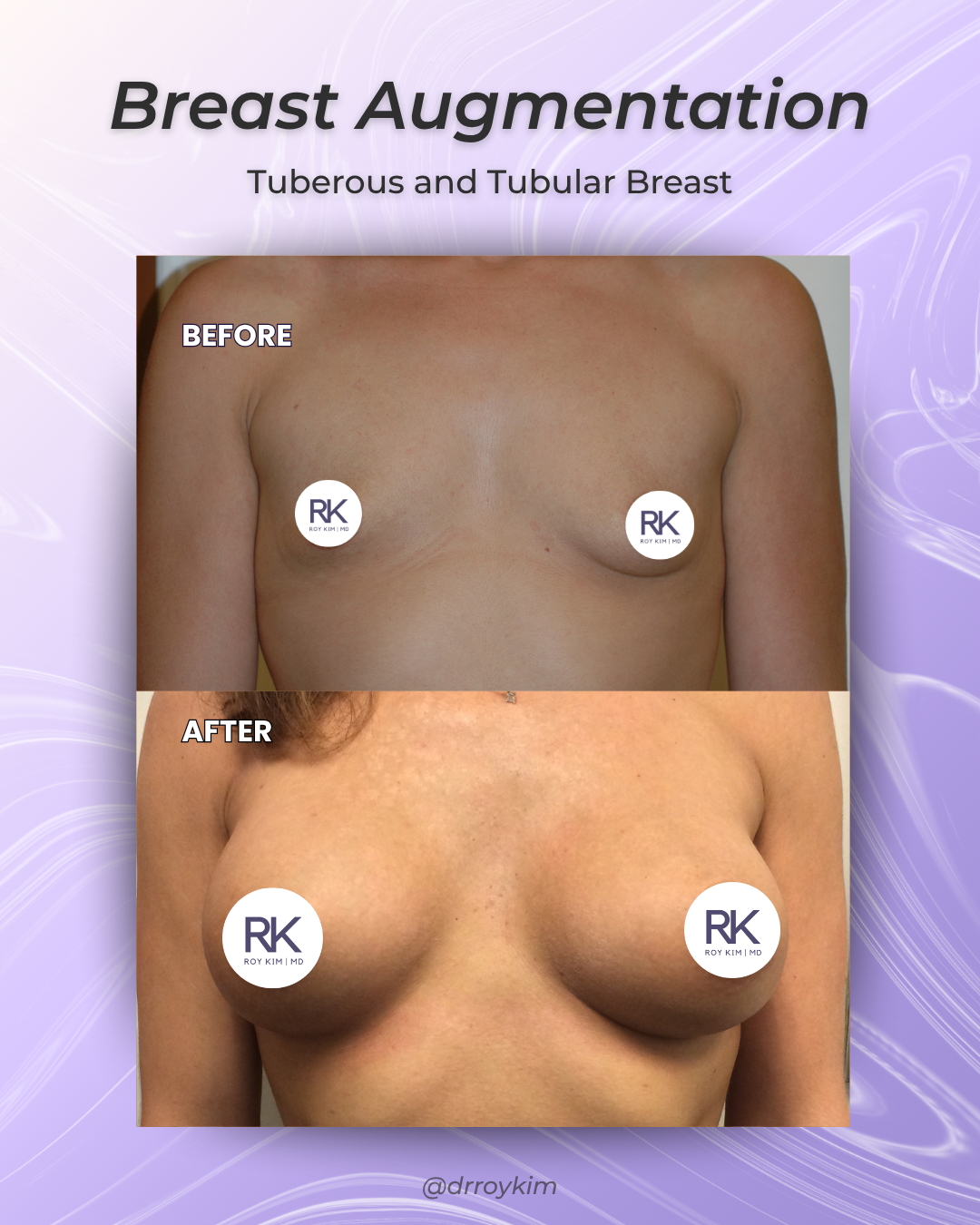
before and after tubular breast
1. What Tubular Breasts Are (and the Story I Hear Most Often)
Tubular breasts develop during puberty. The breast tissue doesn't expand the way it should. Tight bands of connective tissue at the base clamp down and prevent the breast from filling out. Instead of growing into a rounded shape, the tissue gets forced forward and upward. The result is a breast that looks narrow, constricted, sometimes tube-shaped, often with a puffy or swollen areola.
The story I hear at almost every consultation goes something like this. A patient in her twenties or thirties tells me her breasts have looked different since she was a teenager. They're small and saggy even though she hasn't had children, hasn't gained or lost significant weight. The areolas are large, sometimes puffy or domed. She's spent years thinking her breasts are "weird" but never knew there was an actual diagnosis.
Tubular vs. tuberous: You'll see both terms used interchangeably online. Technically, a tubular breast has some tissue but looks elongated, like a tube hanging over a fold that sits too high. A tuberous breast is generally smaller and flatter. In practice, the conditions overlap and the surgical correction is similar for both.
2. The 10 Signs I Evaluate During a Consultation
Not every patient has all ten of these features. I've seen cases where someone has three or four signs mildly and another patient has seven or eight severely. Here's what I'm looking at:
A narrow, constricted breast base. The "footprint" of the breast on the chest wall is tight instead of wide and circular. This is the hallmark sign.
The breast fold sits too high. The crease under the breast hasn't dropped to where it should be, so the lower half looks short and underfilled.
Areolar herniation. This is the "puffy nipple" look. The skin at the base is so tight that breast tissue pushes through the path of least resistance, which is the thin skin of the areola. I'd say this is the feature that bothers patients the most before they come see me.
A tubular or conical shape rather than the teardrop contour you'd expect
Those first four signs are the ones I notice within seconds of a physical exam. The remaining features vary more from patient to patient:
Significant asymmetry. It's common for one breast to be tubular while the other develops normally. This makes the correction trickier because you're essentially performing a different procedure on each side.
Minimal breast tissue, enlarged areola, and a wide gap between the breasts. These three tend to travel together. The narrow base means less volume, the herniation stretches the areola, and the constriction pushes the breasts further apart.
Tight lower pole skin that prevents the breast from rounding out naturally below the nipple
Drooping despite small size. This one confuses patients. They think sagging means too much tissue, but with tubular breasts it's the opposite. There isn't enough lower pole support, so even a small breast droops.
3. Why a Standard Augmentation Won't Fix This
So what happens if you skip the tissue release and go straight to an implant? I've seen it. Patients who went to another surgeon, got a standard augmentation, and came to me frustrated. The breast was still narrow, still constricted, with the implant sitting high and the tissue bunching around it.
The problem is structural. Those tight tissue bands at the base are still there. Dropping an implant behind them is like trying to inflate a balloon inside a rubber band. The volume goes somewhere, but not where you need it.
If a surgeon proposes a straightforward augmentation without mentioning tissue release, get a second opinion.
[LINK: Breast Augmentation Hub]
4. How I Correct Tubular Breasts: The Surgical Plan
Every case requires a custom plan, but most of my tubular breast corrections involve the same core elements.
I start with an areolar incision. This is my primary access point because it puts me right where I need to be: at the breast tissue itself. It also lets me reduce an enlarged areola at the same time. Two problems, one incision.
From there, the most critical step is the tissue release. I make internal cuts in the breast tissue, what I call "pie cuts," from roughly the 3 o'clock position to the 9 o'clock position along the lower half of the breast. Picture the spokes of a wheel radiating outward. These cuts allow the constricted tissue to relax and spread out, giving the breast a wider, more natural base. Without this step, you're fighting the anatomy.
Then comes implant placement. I use silicone gel for tubular breast correction because it has more internal support than saline. That structure helps create a rounded shape at the bottom of the breast, right where the constriction used to be. When you're reshaping a tight lower pole, you need an implant that works with you, not against you.
In most cases I also lower the inframammary fold to its proper position, which gives the lower pole room to fill out. And for some patients, I'll add fat grafting along the implant edges and lower breast to soften transitions. I either do this during the primary surgery or save it for a secondary procedure after healing.

Diagram or illustration showing pie cut technique and tissue release concept
5. Recovery: The Timeline Patients Need to Know
Two timelines matter here. The short one: back at a desk in one to two weeks, back at the gym in six weeks.
The long one is what most patients underestimate.
The number I want you to remember is 6 to 12 months. That's how long it takes for the tissue to settle into its new shape. I know that sounds like a long time. It is. But the remodeling process after tissue release takes longer than a standard augmentation recovery, and tubular breast tissue is unpredictable.
I had a patient from Pacific Heights who was convinced at four months that something was wrong because one side looked tighter than the other. By nine months, both sides had settled beautifully. Another patient who commuted from Marin for her follow-ups kept asking me if the lower pole was going to round out more. It did.
Some patients benefit from a revision about a year out. A little fat grafting, a scar touch-up, sometimes done in the office. Not everyone needs it, but I'm upfront about the possibility at consultation.
6. Breastfeeding After Tubular Breast Correction
Younger patients ask about this in almost every consultation, and they should. The surgery is designed to preserve breastfeeding function. The implant goes beneath the muscle, separate from the milk ducts, and the tissue release doesn't target glandular tissue.
Here's the nuance though. With tubular breasts, the glandular tissue was already underdeveloped before you walked into my office. I'm not making breastfeeding harder than your biological baseline, but I won't guarantee the condition didn't already limit how much functional gland you have. That's an honest conversation I have with every patient thinking about pregnancy down the road.
[LINK: Breast Augmentation and Breastfeeding]
Myths About Tubular Breast Correction
"A regular breast augmentation will fix it." This is the myth I run into the most, and sometimes it's coming from other surgeons. Without releasing the constricted tissue first, an implant behind a tubular breast looks like a ball stuffed in a sock. Structure before volume.
Another one I hear: tubular breasts are extremely rare. They're not. Plenty of women have mild forms and never realize there's a clinical name for it. The condition is underdiagnosed, not uncommon.
And the idea that results look unnatural? When the correction is done properly, with tissue release, the right implant, and fat grafting where needed, these are some of the most dramatic and natural-looking outcomes in breast surgery.
Frequently Asked Questions
-
The classic combination is breasts that look small and saggy even though you've never been pregnant or had major weight changes, with enlarged or puffy areolas and a tubular rather than round shape. You don't need every sign to have it. A board-certified plastic surgeon experienced with tubular breast correction will tell you during a physical exam. If you're reading this article and nodding along, it's worth a consultation.
-
Usually not. Most insurance companies classify it as cosmetic. I've had a few patients with severe asymmetry get partial coverage, but that's the exception.
-
This is a question I get a lot, and with tubular breasts it matters more than in a standard augmentation. Silicone gel has more cohesion and internal support, which is what I need when I'm reshaping a tight lower pole. The implant has to hold a rounded shape and help push the released tissue into a natural contour. Saline is softer, less structured, and doesn't do that job as well. The specific size and profile depend on your anatomy, the severity of constriction, and the result you're going for.
-
Between 2.5 and 4 hours under general anesthesia. Asymmetric cases where each side needs a different approach run toward the longer end.
-
Possibly. And I'd rather be honest about that upfront than surprise you later.
Tubular breast tissue is unpredictable in how it heals after release. That isn't something any surgeon controls. If a revision is needed, it's typically about a year after the first procedure and it's often something smaller: fat grafting to smooth a contour, a scar refinement, or a minor adjustment I do in the office. Not every patient needs it. But going in knowing it's a possibility makes the whole process less stressful.
-
Better than most patients expect. The primary scar runs around the areola, and the natural color transition between areolar and breast skin camouflages it well. Some patients have a small additional scar along the new inframammary fold. Most patients tell me at their one-year follow-up that they're pleasantly surprised at how well things faded.
Summary
Tubular breast correction goes well beyond placing an implant. It requires releasing constricted tissue through pie cuts, selecting a silicone gel implant that supports the lower pole, reducing the areola, and often adding fat grafting for a smooth result. Recovery asks for patience, and some patients benefit from a smaller revision down the line. For women who have lived with this condition since their teens, the change is one of the most meaningful outcomes I see in my practice.
Schedule a Consultation
If you think you have tubular or tuberous breasts, I'd be glad to evaluate your case. I see patients at my San Francisco office (450 Sutter Street, Suite 1440) and my Alameda location (1403 Park Street). Consultations run about 45 to 60 minutes, and I do the entire visit personally. Call 415-362-1846 or email info@drkim.com. If you're unsure whether you're a candidate, send photos to my Patient Care Coordinator and I'll give you an honest answer before you come in.
Follow and Connect with me on my social media!